|
Rotator Cuff Tears
|
Description
|
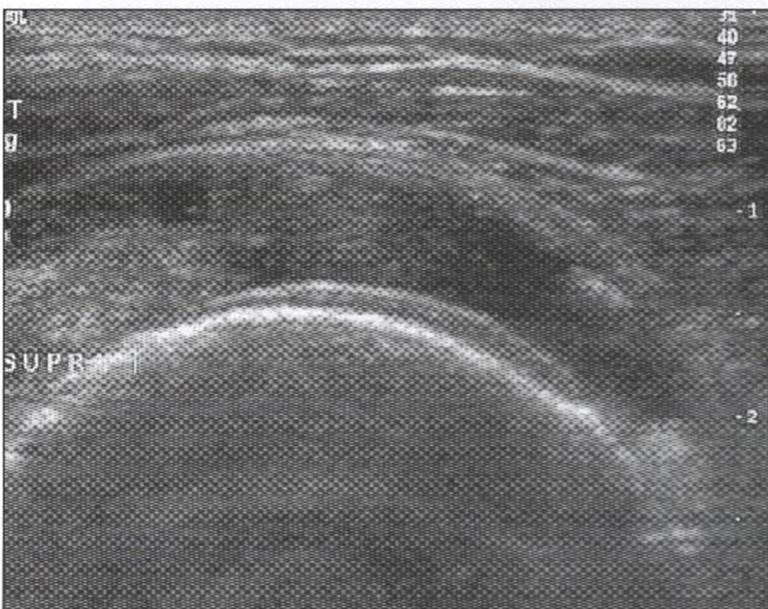
Sonographic Appearance
|
Sonographic Image
|
|
full thickness
|
-a defect that allows communication between the SASD and the glenohumeral joint
- full-thickness tear that is focal may be termed an incomplete full-thickness tear ( OR a free edge tear-where the supraspinatus tendon that lies immediately adjacent to the anterior interval and bicepts tendon tears away) -a tear that involves the entire width of a tendon may be termed a complete or full-width full-thickness tear (OR a masive tear- complete absence of the supraspinatus and possible propagation into the infraspinatus or subscapularis) |
-incomplete tear-tendon fibers are disrupted by a well defined hypoechoic or anechoic abnormality from the articular to bursal side, cortical abnormalities, cartilage interface sign (with small tears there is no volume loss and with large tendons volume loss is apparent)
-free edge tear- loss of the normal supraspinatus tendon substance, widening of the gap between the biceps tendon and supraspinatus tendon and exposure of a bare area of bone and cartilage where the tendon previously attached (may also see the SASD bursa sag into the space created by the tear and it may or may not be filled with excess fluid) -massive tear- complete non-visualization of the tendon, irregular humeral head defects at the supraspinatus attachment site, bony changes in the upper portion of the bicipital groove which becomes irregular and deep, secondary bicipital tendonopathy and which can later become frayed, the deltoid muscle and the SASD bursa sit on the humeral head |
|
|
partial
|
-a tear that does not completely traverse the tendon it involves
-involve either the articular (articular surface tear), bursal surface (bursal surface tear) of the tendon, or it can be localized within the tendon (interstitial/ intersubstance tear) -articular surface tears are more common than bursal surface tears |
-articular surface tear-fluid seen in between the articular surface of the humerus head and the tendon (cartilage interface sign)
-bursal surface tear-fluid is seen in the SASD space superior to the tendon, can extend to the greater tuberosity with or without cortical abnormality, tendon thinning and volume loss, deltoid/SASD dipping, SASD synovial fluid and increase echogenicity -interstitial tear- normal supraspinatus tissue can be identified anterior to this tear and normal supraspinatus and/or infraspinatus posterior, no convexity loss or volume loss |
|
|
acute
|
-acute tears usually occur more proximally on the supraspinatus
|
-commonly they are anechoic and are filled with fluid
-may or may not have associated cortical irregularity, depending on the age of the patient and the state of the underlying rotator cuff |
|
chronic
|
-chronic supraspinatus tears usually occur distally on the supraspinatus
|
-cortical irregularity of the greater tuberosity may be seen, which is an important indirect sign of supraspinatus tendon tear
-the distal torn tendon may be tapered without adjacent fluid but possibly with isoechoic or hyperechoic synovial hypertrophy |
|
**most rotator cuff tears involve the supraspinatus tendon, although they may extend posterior to involve the infraspinatus and anterior to involve the biceps reflection pulley and subscapularis tendons
(Jacobson, 2007)
(McNally, 2005, pg. 44-52)
(Thomas, 2014)
(McNally, 2005, pg. 44-52)
(Thomas, 2014)
|
Pathology
|
Description
|
Sonographic Findings
|
Sonographic Image
|
|
bursitis
|
-inflammation of the bursa,
-caused by trauma, arthritis, gout (complex from of arthritis) or synovial disease -usually associated with supraspinaus tendonitis, subacromial impingement, and rotator cuff tears |
-starts as an effusion (usually in the SASD bursa)
-may appear anechoic or hypoechoic from simple fluid, or it may range from hypoechoic to hyperechoic as a result of complex fluid or synovial hypertrophy -color or power Doppler imaging may differentiate complex fluid from synovitis because blood flow suggests synovial hypertrophy |

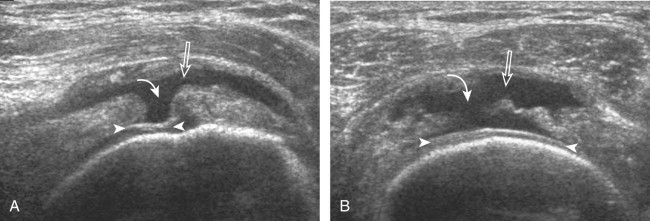
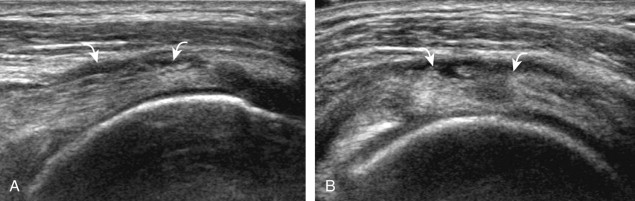
Figure 26. This is a sonographic image of the short axis of the biceps tendon demonstrating distention of the SASD bursa filled with anechoic fluid and heterogeneous synovial hypertrophy. B-biceps tendon, white arrows-pointing to the SASD bursa.
|
|
calcific tendonitis
|
-a chronic inflammation of a tendon resulting from an accumulation of calcium deposits primarily as calcium hydroxyapatite deposition, possibly from decreased oxygen tension and fibrocartilaginous metaplasia
-the underlying rotator cuff is typically intact -the supraspinatus is most commonly involved but other rotator cuff tendon involvement is not unusual |
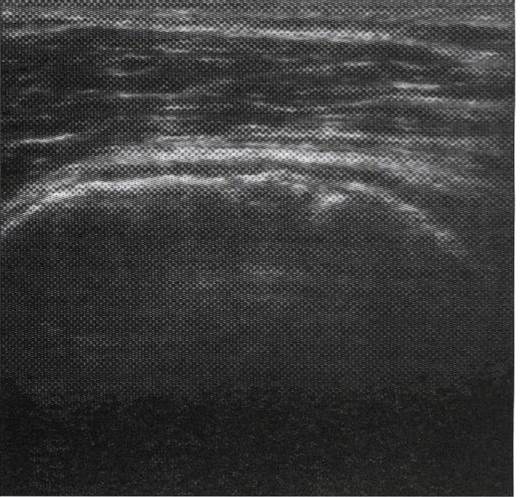
-although their appearance may vary, the calcific deposits most commonly are hyperechoic with posterior acoustic shadowing
-small calcifications may be linear along the axis of the tendon fibers, whereas others have an amorphous appearance or are globular with minimal or no shadowing -cortical erosions and osseous involvement may also be present -when calcific deposit echogenicity is isoechoic to tendon without shadowing, the amorphous echotexture during real-time scanning can be identified, and this replaces the normal fibrillar tendon appearance -increased flow on color and power Doppler imaging around the calcifications may be evident -calcifications may be identified at the bursal edge of the involved tendon with possible extension into the subacromial-subdeltoid bursa |
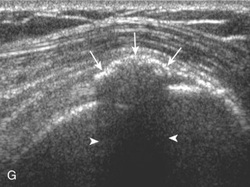
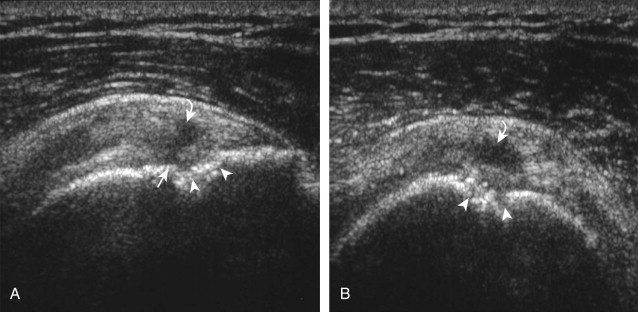
Figure 27. This is an image demonstrating the sonographic appearance of a supraspintus tendon in long axis with clacific tendonitis. Although appearance may vary, this is a classic case of calcific tendonitis. Arrows-pointing to the calcium deposit, arrowheads-pointing to the posterior shadow created by the calcium deposit. Adapted from "Fundamentals of Musculoskeletal Ultrasound" by Jacobson, A, Jon, 2007, Wrist and Hand Ultrasound, 5. Copyright by Elsevier, Inc.
|
|
supraspinatus tendonosis (tendinopathy)
|
-a degenerative process with eosinophilic, fibrillar, and mucoid degeneration and possible chondroid metaplasia
-no active inflammatory cells |
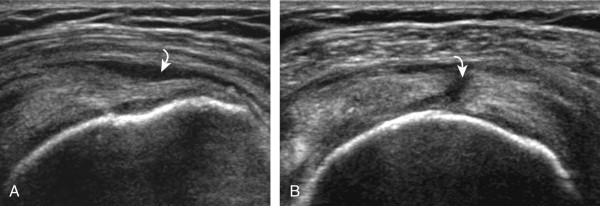
-heterogeneous, somewhat ill-defined, hypoechoic area in the tendon without a tendon defect
-unlike tendon tear, tendinosis is usually less defined, it may be associated with tendon swelling, and it is usually not associated with adjacent cortical irregularity of the greater tuberosity -diffuse tendinosis may cause the entire tendon to appear hypoechoic, equal in echogenicity to adjacent muscle -unlike a massive tendon tear, a normal convex superior surface of the supraspinatus is seen |
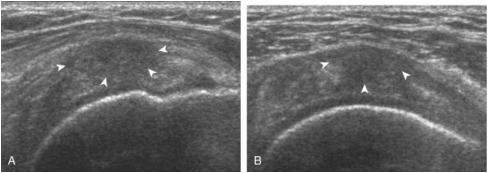
Figure 28. This is a sonographic image demonstrating a supraspintus tendon in long axis with focal tendonosis. White arrowheads-pointing to the ill-defined hypoechogenicity and mild tendon swelling. Adapted from "Fundamentals of Musculoskeletal Ultrasound" by Jacobson, A, Jon, 2007, Wrist and Hand Ultrasound, 5. Copyright by Elsevier, Inc.
|
(Jacobson, 2007)
(McNally, 2005, pg. 69-73)
(Thomas, 2014)
(McNally, 2005, pg. 69-73)
(Thomas, 2014)
Partial Tears
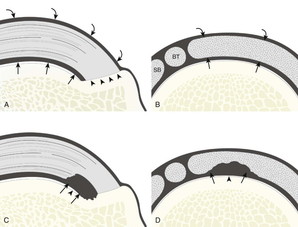
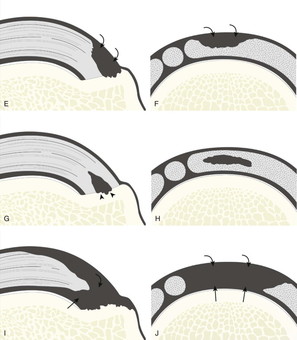
Figure 29. Supraspinatus tendon tears. Illustrations in long axis (A) and short axis (B) to the supraspinatus tendon show the articular (arrows), bursal (curved arrows), and greater tuberosity (arrowheads) surfaces of the supraspinatus tendon. C and D, Articular-side partial-thickness tears (black) contact the articular surface (arrows) and hyaline cartilage (arrowhead). E and F, bursal-side partial-thickness tears (black) contact the bursal surface (curved arrows). G and H, Intrasubstance tears (black) reside within the tendon not in contact with the articular or bursal surface, although isolated greater tuberosity contact within the tendon may be seen (arrowheads). I and J, Full-thickness tears extend from articular (arrows) to bursal (curved arrows) surfaces. Note that all types of tears may contact the greater tuberosity, associated with bone irregularity. BT, biceps tendon; SB, subscapularis tendon. Adapted from "Fundamentals of Musculoskeletal Ultrasound" by Jacobson, A, Jon, 2007, Wrist and Hand Ultrasound, 5. Copyright by Elsevier, Inc.
